
How robust are the clinical signs of FND such as Hoover’s sign and the tremor entrainment test. These seem important because this is how the diagnosis is made. If they aren’t reliable then how reliable is the diagnosis?
The diagnosis of FND does depend on finding positive evidence of the diagnosis on assessment. It is not about doing a lot of tests such as brain scans and nerve conduction tests and showing they are normal.
There are many positive clinical signs described and there isn’t space to describe them all here. They are described on each of the relevant pages of the website.
Some of these are listed in the panel on the next page taken from a review article on FND written by an international authorship1.
Few physical signs in neurology are 100% reliable, yet neurologists have used them effectively for hundreds of years to make diagnoses that are meaningful and group people in to conditions that benefit from common treatments.
For example, Parkinson’s disease has been a clinical diagnosis for most of the last 100 years based on finding a typical type of tremor of the arms at rest, a certain kind of stiffness and slowness of movement. James Parkinson recognised that combination in 1817 and what he observed has turned out to be remarkably consistent. On their own these features are not that reliable. You can have tremor, stiffness and slowness for lots of reasons, but the combination in the right clinical context increases the accuracy.
Usual brain scans such as MRI and CT are typically normal in Parkinson’s disease, just like in FND. Now that we have other ways of diagnosing Parkinson’s disease (i.e. DAT scans) – these are helping with some cases, although in others they aren’t helpful because we meet people who clinically clearly have Parkinson’s disease, but have a normal DAT scan.
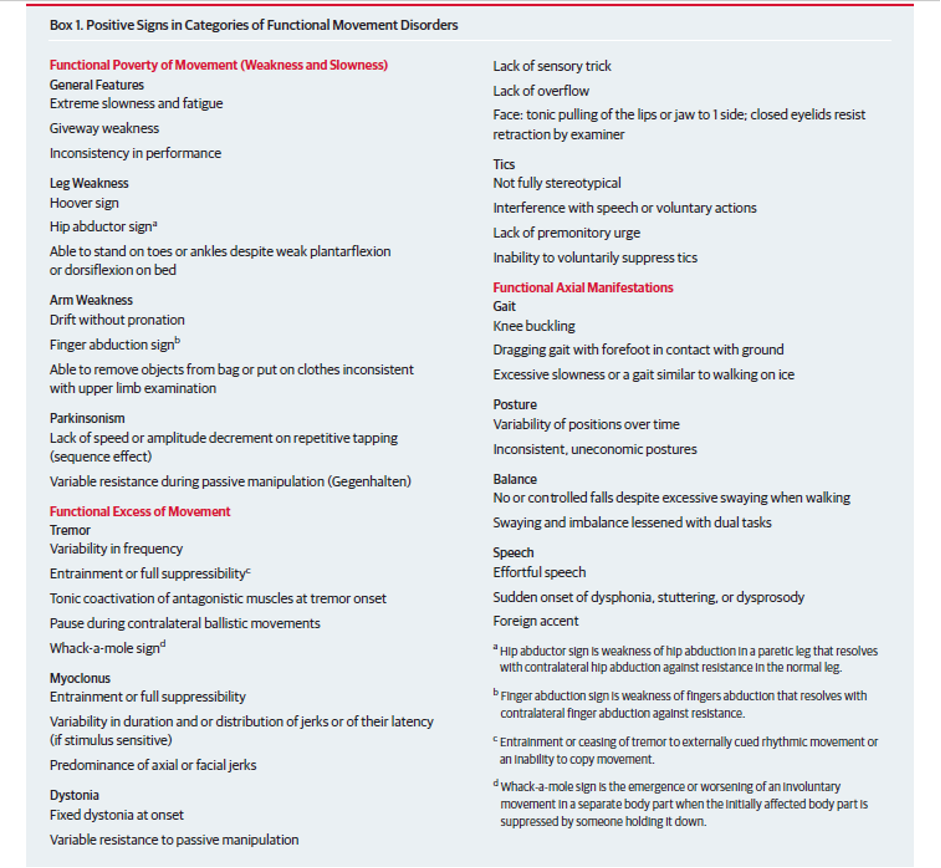
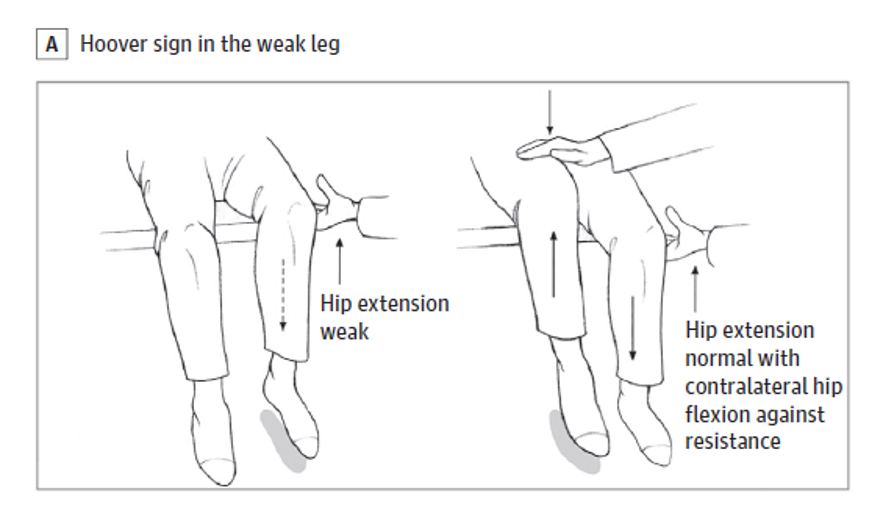
For FND, each of the signs in the panel has a varying degree of reliability. Studies looking at them show that they can discriminate between patients who have functional leg weakness and patients who have other neurological diseases, even when doctors don’t know what the diagnosis is, in advance2,3. Some of them, like Hoover’s sign, perform well in these tests and for others we have less data or there needs to be more caution.
There is no such thing as a clinical sign which is always reliable for FND, or indeed most disorders – whether neurological or psychiatric. Each sign needs to be put together with other signs and the clinical story to come to a rational diagnosis. A skilled neurologist needs to learn how much weight to place on each of their findings and investigations and come to a conclusion. That conclusion may be that they do know what is wrong because they recognise the whole pattern, like Parkinson’s or someone with FND. Quite often in neurology, it’s not possible to come to a conclusion, the doctor should then say they aren’t sure. In other patients there may be more than one diagnosis. Its common for example for patients to have both a neurological condition like multiple sclerosis AND FND.
This is how medicine works. It is a science but also a skill, and therefore can be prone to human error.
References:


We will be re-directing you to the University of Edinburgh’s donate page, which enable donations in a secure manner on our behalf. We use donations for keeping the site running and further FND research.
